Dental/Cancer Connection by Dr. Gerald H. Smith It is estimated that 70% of all medical illnesses are directly or indirectly caused by human intervention in the dental structures (teeth and jawbones). This includes: impacted teeth, infected root canalled teeth, new and recurrent decay around old fillings, cysts, bone infections in areas of previously extracted teeth, granulomas and areas of bone condensation to osteitis represent some of the more common factors. Boyd Haley, Ph.D., a researcher, at the University of Kentucky has estimated that 75% of root canalled teeth are infected. Another researcher, Hal Huggins, DDS, has shown that the toxins liberated by infected root canalled teeth are almost 1000 times more toxic than botulism. Botulism is the most toxic substance known. According to the observations made by the internationally recognized medical researcher, Yoshiaki Omura, MD, all cancer cells have mercury in them. Since mercury is the second most toxic substance on this planet, its presence provides a strong initiating factor for disrupting cell function. An effective approach to treating cancer MUST include: - Detoxification (heavy metals, chemicals, etc.)
- Boosting the Immune System (anti-oxidants)
- Regeneration of damaged tissues (organic nutrients)
- Destruction of cancer without destroying the body
- Psychological Healing
Cancer:
A Second Opinion, Chapter 8, Focus on Foci by Josef Issels, 1999 My clinical experience has produced evidence of a causal connection between dental foci and tumour development, and in this respect, the results obtained with the aid of an infra-red test are especially significant. Any inflammatory disease focus creates on its corresponding skin surface a pathological increase of infra-red emission; the higher the activity of the focus, the more pronounced it is. Using an infra-red sensitive instrument (Schwamm's infra-red toposcope), the intensity of this emission can be continuously monitored and measured. Observation shows a close interrelation between the infra-red emission of head foci and that of the neoplasial region. That is, after treatment, a decrease in the infra-red activity of dental foci was as a rule accompanied by a decrease in infra-red emission over the tumour areas. From this it is clear that the advisable treatment for devitalized teeth is extraction. But even this is not always enough. My experience has further shown that also living teeth may sometimes be so damaged that their pathogenic potential almost equals that of devitalized teeth. For instance, latent chronic pulpitis may arise in a tooth that appears outwardly healthy, thus having a focal effect. The diagnosis and treatment of dental foci remains generally unsatisfactory. A survey conducted at my clinic found that, on admission, ninety-eight percent of the adult cancer patients had between two and ten dead teeth, each one a dangerous toxin producing "factory". Very often we are confronted with X-ray negative dead teeth, root remnants, and residual ostitis which had not been diagnosed and therefore had not been removed. Only total, thorough dental treatment will really succeed in giving the body's defense a chance. In addition to X-ray diagnosis, it is therefore necessary to use other diagnostic aids, such as infra-red techniques, tests, to estimate tooth vitality and periosteal resistance, and other electrometric methods. The diagnosis of foci in teeth had been greatly improved by electro-acupuncture. It is now possible to differentiate foci not only with regard to their type and position, but also to their virulence and pathogenic efficacy. The result of focus treatment can consequently be observed and improved, before, during, and after dentistry, to an extent never known before (Kramer). If total treatment is to be performed, it is necessary to remove not only any devitalized teeth but also any hidden dental foci remaining in the jaw. Further, total removal of devitalized teeth and their roots must not be the end of the dentist's activities. Each alveolus - the tooth's socket in the jaw - should be radically cleared down to the healthy bone. In that way the development of the residual ostitis or of a cystoma may be prevented. It is not only the tooth which may be a focus, the but the adjacent tooth-fixing apparatus as well. There are four different ways by which dental foci - and indeed all foci - can affect the organism and contribute to the development of secondary damages: 1. The "neural" way of affecting the organism. When a focus develops anywhere in the transit tissues, the mesenchyme, the process is centripetally projected from the terminal neural organs around the irritated area, along the neural ducts, up to the corresponding control cells within the central nervous system. The irritation originating from a focus can, under certain conditions, trigger off the mechanism of a neural dystrophy - a slow degeneration - which may show itself in localized effects in other areas, but also in a generalized dystrophic disturbance. Ferdinand Huneke, the founder of neural therapy, discovered over forty years ago that injection of a local anaesthetic near a primary focus may immediately remove any symptoms of distant disease induced by the focus. This effect - the second-phenomenon - usually takes place only a few seconds after the anaesthetic injection, and lasts for hours, days, or even for a lifetime. Naturally the improvement occurs only in those regions influenced by the injected focus. Nevertheless, the measure has therefore a remarkable diagnostic value as well. 2. The "toxic-way" of affecting the organism. The toxic activity of odontogenic foci is probably far more perilous for the organism than their neural effects. The mechanism of this distant toxic activity, as well as the characteristics of the toxic compounds involved, have been largely ascertained. Odontogenci compounds are the gangrenous contents of an inflamed pulp cavity and its adjoining spaces. It consists of detritus and decaying, formerly vital substrates which have been necrobiotically altered - commonly found in tissues destroyed by inflammation, liquefaction and microbial putrefaction. There is hardly a carcinogen which so completely fulfils these conditions as do thio-ethers [a type of dental toxin]. Incessantly, from the moment the pulp is removed, hour by hour, year by year, minimal amounts of these most virulent of all the odontogenous toxins will be released into the circulation - minimal doses, but nevertheless sufficient to more or less totally paralyse the aerobic action of the cell. The close interlacing of the lymphatic and endocrine systems in the head, make it unavoidable that brain cells are more intensively toxified by the circulating focogenous agents and may suffer particularly heavy damage. The lymph ducts of the head region join Waldeyer's tonsillar ring, and if there is such congestion, waste fluids will be pressed through the porous base of the skull into the lymphatic spaces of the brain. Toxogenous changes, especially within autonomic nuclei, are regularly found in cancer patients, as verified in the 1930s by Muehlmann (USSR), and they may be a consequence of a life-long inhibition of cerebral aerobiosis due to focogenous intoxication. The cerebral damage (diencephalosis) and the subsequent loss of vitality in cancer patients is accompanied by the number of other symptoms. The emission of hypothalamic energy impulses, recordable by a Voll's electro-acupuncture device, are reduced in patients with focal disease. The autonomic vigour is relaxed, creating "regulation rigidity": carcinomas tend to parasympathicotonic derailment; in sarcomas and systemic diseases, as a rule the opposite is found - sympathicotonic derailment (Regelsberger, Gratzl-Martin, Rilling et al). the diurnal, circadian regulation of the acid-base balance is lost (Sander). At the same time, there will exist a distinct inhibition of other diurnal control functions, for instance of blood sugar, cholesterol, and mineral metabolism, and many other metabolic parameters are greatly restricted (Hinsberg). The lack of vigour and control efficiency is not, of course, without effect on the patient's psychic condition. Vegetative disorder is therefore generally accompanied by neurasthenic dystonia - characterized by the diminishing vitality and autonomic instability. 3. The "allergic" way of affecting the organism. The toxic effects of thio-ethers overlap those caused by higher-molecular odontogenous toxins as already described. Antibodies are formed to fight these substances, eventually leading to the destructive processes in toxified cells. Since the organ-destroying antibodies or defence enzymes are excreted by the kidneys, they can be diagnosed in the urine by the abderhalden test. In this way we can precisely deduce, in most cases, which organs have suffered secondary damage (Abderhalden, Dyckerhoff et all). The extent of secondary lesions can also be demonstrated indirectly by vaccine treatment. Using desensitizing vaccines made from focogenous agents, reactions are caused in regions affected by distant focal effects which may become evident in regional as well as general symptoms. It is thus clear that the development of cancer disease is, in more ways that one, closely linked with focal events. 4. The "bacterial" way of affecting the organism. Bacterial dissemination from primary dental foci as a rule takes place with barely perceptible symptoms, and may be followed by the formation of "secondary foci" in other regions. These include, inter alia, foci in the paranasal sinuses, gall-bladder, appendix, prostate, and renal pelvis. The dentists' task is only secondarily cosmetic; primarily it must be preventive and curative. The over-riding consideration must not be conservation of the tooth but preservation of its vitality. If this is impossible, even the most beautiful crown must not delude us that the lifeless tooth beneath is anything other than a "corpse in a golden coffin", whose decomposition toxins slowly but surely are destroying the organism (Bircher-Benner). Other foci in the jaw, for instance ostitis, cysts, foreign bodies, gingivitis, and malposition of teeth may also develop focal effects. It goes without saying that these foci and centers of irritation must be removed. The dentist should always remember that he has a vital role to prevent the development of chronic illness and, most important of all, to decisively reduce the hazard of cancer. Now let us turn to tonsillar foci. Chronically inflamed tonsils are primary head foci which sometimes have an even more damaging effect on the organism as a whole than dental foci. They can participate in the development of chronic illness, including cancer, by the four ways already described for dental foci: by neural, toxic, allergic, and bacterial means. There are also similar connections between the development of cancer and tonsillar foci as there are between cancer and dental foci. For instance, after removing the tonsils, there is a decrease of infra-red radiation over the tumour, and sometimes even a shrinking of the tumour.
Researcher Robert Jones' Presentation. . . "As I have explored the causes of cancer it has become apparent that the real cause of cancer is genetic protein based, in other words, toxic inhibition of proteins within the cell structure allows or encourages a cell, or group of cells, to become malignant [cancerous]. The International genome project flatly states that all cancers are caused by one or more of 3 things: 1.
Radiation 2.
Chemical Toxins 3.
Spontaneity I have concentrated my efforts to uncover the cause of cancer as chemical toxins as we have no way to control or measure the rate of radiation exposure. I started on the conquest of exploring chemical toxicity and its relationship to protein inhibition several years ago. In the process of my research, a huge amount of toxins have been looked at. As we narrowed the search to a protocol of daily or chronic exposure, at the top of the list were compounds of known carcinogen and neurotoxins, these toxins being classified as thio ethers. The most significant of these thio ethers is dimethyl-sulfide. Although small in amounts of exposure, the average inhibition of ability to bind to the cellular membrane came to a startling conclusion of more than 90% inhibition as an average for all three proteins. To
distinguish which toxins in particular, we tested 36 types on Affinity Labeling gels. Specifically, as we set the protocols for this research project we used toxicity samples from over 900 extracted root canal teeth as a composite and over 4000 bone fragments obtained from biopsy samples as a separate composite. Root canal toxins and cavitation [broken tooth] toxins were tested separately to determine how each toxin individually inhibited the binding ability of the protein. Establishing published cellular weights (amounts) of these proteins, we proceeded to inject Affinity Labeling gels with amounts of human protein as to the stated amount found in each individual cell. So, therefore, using toxins extracted from human samples and human proteins, we were able to exhibit extreme or severe inhibition of these individual proteins by chronic exposure to these toxins. We then ran additional types on the same Affinity Labeling gels to determine the effects of blio toxins (fungi) and also mercury from dental amalgam. As you will note during my lecture, the cavitation toxins from a composite of 100 or more cavitations was much more toxic than root canal toxins. I'd
like to show you in our basic DNA, we have the chromosome ladder as illustrated in blue and protein in green with amino acids in yellow. Notes
in
red are our
comments
that perhaps can clarify points for non-scientific readers:  | The
inhibitions I will demonstrate will have a serious
effect on the protein's ability to function in the nucleus of the cell and the downstream effects of these inhibitions and how they affect the cellular functions will be noted. Inhibitions
refers to how cancer-preventing proteins are inhibited from fulfilling their role. You will see that when the condition is corrected, the proteins can restore their ability to protect you from tumors. This makes cancer curable and not just a remission state.
|  | I'd
like to talk to you about each protein individually and about how each functions which has been established by the Science of National Genome Research Project.
| | The
proteins that we are going to look at are P54, P21, CDK2 and then we are going to look at a new publication from the University of Michigan published in the Journal of the National Cancer Institute. We will
look
at the inability to bind P27 to P21 and demonstrate how it allows the cancers to metastasis.
Notice
here that other studies from reputable organizations are involved in this research. | | | What
is P53? P53
is specifically a tumor suppressant protein. It has been defined as a normal function of P53 to be anti-cancer.
While type P53 proteins introduced into cells were found to be growth suppressant, P53 is found rarely in a tumor cell, while it is very prolific in normal healthy cells. When it is found in a malignant tumor, it is found sparingly and in an inhibited state as we will demonstrate and therefore its ability to bind in the cellular membrane is greatly reduced. When P53 is normal or not inhibited, tumor growth or start is depressed. The
point
being made here is that the P53 is a protein known to suppress tumor development. In other words, it is an anti-cancer protein when it is allowed to function in a normal manner.
| | | Amino
acids are an important class of organic compounds that contain both the amino (_NH2) and carboxyl (_cooh) groups. Of these acids, 20 serve as the building blocks of proteins. These amino acids are inhibited from binding to the chromosome ladder and or just one of the examples of damage incurred by these dental toxins. The
very building blocks of proteins are inhibited by the dental toxins. This is one factor involved in the "wasting" process often seen in terminal cancer cases.
| | This
is the nucleotide protein gel before developing. | 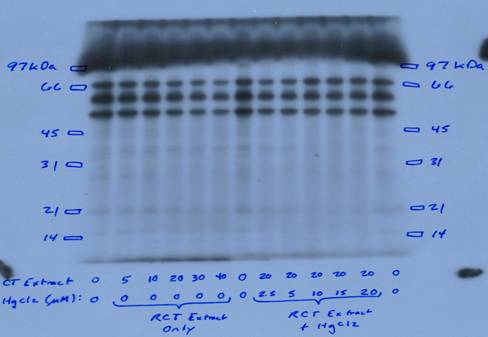 | 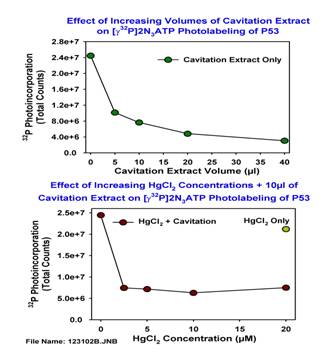 | If
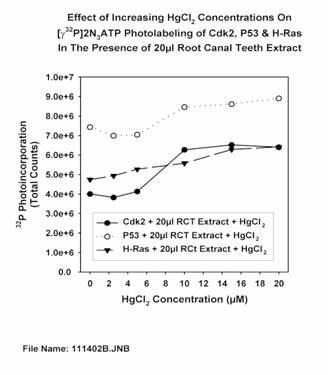
you will note, we have a graph that is printed out with a Hewlett Packard Phosphorescence measuring device as it measures radioactive light. This is non-subjective analyzation of inhibition of proteins ability to bind and function. | 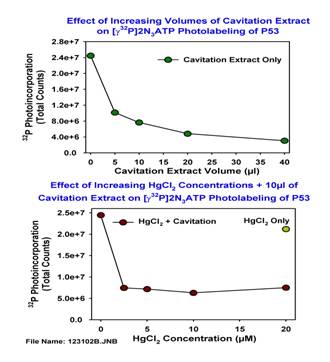 | To
the left vertically is the scale of light reading. The bottom from left to right is the amount of toxin injected into each protein extract. They are shown in micro liters (ul).
| 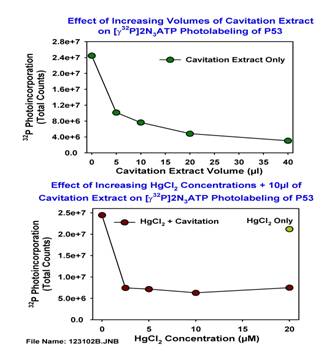 | If
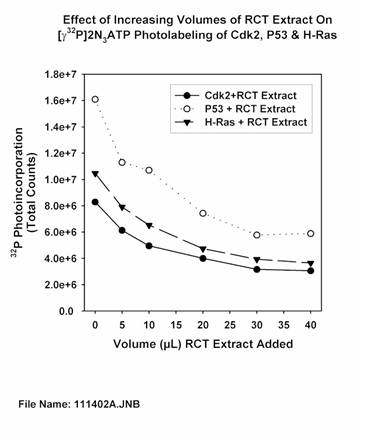
you will note on P53 at 5 ul injection of the cavitation extract, the inhibition is already at 58.5%, any inhibition at over 12% will render functions to be ineffective. What's interesting about this is that at 40 ul they are inhibited at about 85%. A cavitation is a hole in the jawbone that is often (but not always) caused by poor dentistry. Generally these osteonecrotic areas of bones are at the sites of extracted wisdom teeth, but can be at other extraction sites as well. The researcher extracted tissue from these sites to perform the tests.
| 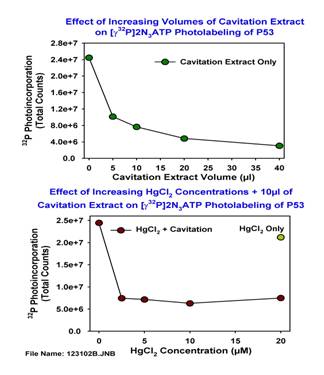 | Then,
we wanted to look at mercury amalgam vapors and what would they do to the inhibition aspects and we were surprised to find that mercury has very little effect in the binding ability to our DNA at this stage of toxicity. In fact, photo labeling increased very slight when 10 ul was added to the cavitation toxins. This is not to say that mercury by itself would not damage these proteins, but did not provide a synergistic effect. So the condition was not exacerbated by the addition of the mercury. We
know mercury is dangerous, but it appears that it is not a direct contributor to the cause of cancer. Mercury, of course, is well known for it ability to depress immune functioning, therefore, it contributes to the body's inability to fight the disease once in progress.
|  | Now
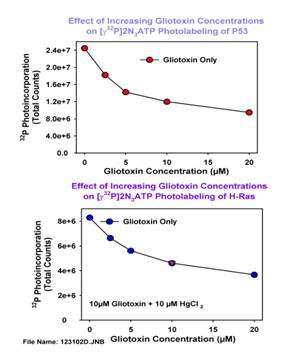
we are looking at a graph of mercury from amalgams added to the Affinity Labeling gel. As you will note, photo labeling of the protein P53 increased with increasing amounts of mercury. So mercury is not the cause of inhibition at this stage.
|  | This
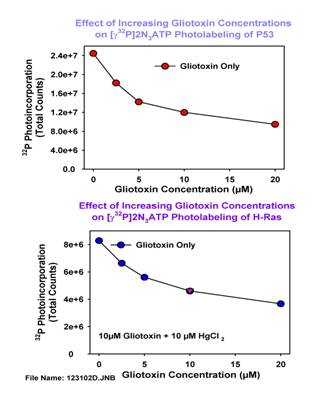
slide shows gliotoxin concentrations produced in micro molar amounts. At 5 um this protein showed 40.7% inhibition. This is a very severe inhibition at very low levels. Even
at very low levels of neurotoxins coming from the jawbones and dead teeth (such as a root canal tooth), severe inhibition can occur.
|  | Of
all three of these proteins, P53 is the top dashed line with the circles. As you note on the chart, P53 from root canal extract inhibits at 29% at 5 ul, continuing on at 40ul at 87.5%. The interesting thing about these toxins is, it is estimated that a molar root canal produces 45ul each 24 hours! All root canals are infected and some do produce more toxins than others. Yes,
root canal teeth! The dentist saves a tooth and sets you up for cancer. There are NO GOOD ROOT CANALS regardless of what the American Dental Association says about root canals. There is no evidence of any double blind study ever made on the safety of rooth canal procedures.
| | | P53
is shown now to be almost totally inhibited. You must remember that Druckrey (Heidelberg) found these dental toxins to be the worlds most perfect carcinogen. Creating an appearance and function of a malignant cell until the carcinogenic dose was reached. Yes,
you
read it correctly--the world's most perfect carcinogen (a substance that is a known cause of cancer) is the dental toxins. Now
we are going to jump over P21 and go to CDK2. | 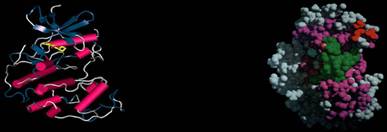 | CDK2
|  | Keep
in mind that CDK2 is a cyclin dependent kinase. To function properly, CDK2 has to bind P21 after P21 has bound P53. We have already demonstrated that P53 is inhibited from binding to the cellular membrane of P21. You
are now seeing the development of the process and why cancer has been a very difficult disease to deal with. Has the millions of dollars in research been given to scientists without the skills to investigate proteins? | | | CDK2'
main function in the GS1 phase is to control cellular mass size or cellular growth and if it is inhibited in ANY AMOUNT this function cannot occur. | 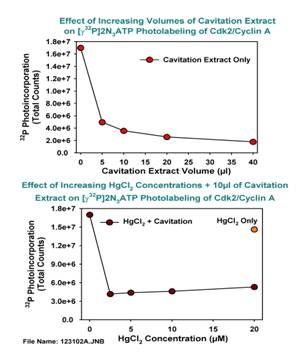 | This
slide, expressed by the Hewlett Packard light source, showing inhibition of CDK2 of cavitation extracts of 5ul to be huge inhibition of 57.6% and that at 40ul, a whopping 89.5%. The lower graph shows basically the same reaction to mercury as shown on P53. | 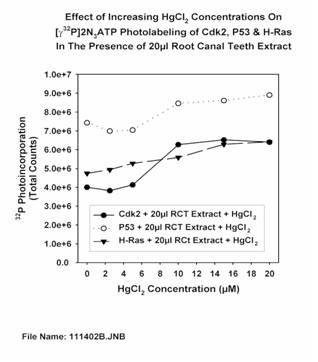 | Now,
we are looking at a graph of mercury from amalgams added to the Affinity Labeling gel. As you will note photo labeling of the protein CDK2 increased with increasing amounts of mercury. So, mercury is not the cause of inhibition at this stage.
|  | Now,
back
to P23.
|  | P21
or H-Ras is the smallest protein yet discovered, but it is the superman of proteins. The primary function of P21 in the cellular structure is to control cell replication and apoptosis. It is also interesting to note that the downstream function of P21 is to control the autonomic immune system. In
saying this, I will return later to this function. The
"superman" of proteins controls cell replication and apoptosis (cell death) which is an important factor in the cure. Cancer cell death must occur to stop the cancer. Rather than destroy with chemicals, which destroys and damages even healthy cells, doesn't it make
more sense to optimize the P21 or H-Ras protein to do its job in the natural cell death of these cells? | 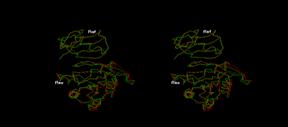 | Protein
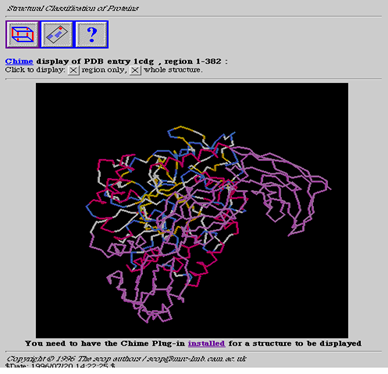
P21 (Ras) & Protein P27 (Raf) Stereo
view of the association between ras-P21, a related protein rap1a, and downstream effector RAF. This is a small part of the cellular signal transduction pathway. These images were obtained by docking ras-P21 and rap1a, each separately, to RAF, based on structural data obtained from x-ray crystallography, and minimizing until the RMS deviation was less than 0.1 angstroms. | | | So,
P21, an important regulatory protein in cell growth and differentiation is a GTPase called Ras. There are 2 cellular switches on P21 that are activated by either GTP or as in the second switch by GDP. When the cellular replication switch is turned on, which is regulated by hydrolyzing GTP, and the switch is turned off by the hydrolyzing GDP as in the second switch. When GTP is bound to the first switch and is inhibited, it cannot hydrolyze GTP. When P21 is unable to hydrolyze GTP the switch remains constant on. So, you have uncontrolled cell replication. The second switch can not glycolyze GDP due to inhibition allowing the cell replication. The second switch can not glycolyze GDP due to inhibition allowing the cell replication cycle to remain full on. The full purpose of the second switch is to turn cell replication off and it cannot function in this capacity due to inhibition. The
second
switch must be activated by removing the neurotoxins from the jawbone which inhibits the P21. This is how to accomplish a cure--not remission! The
downstream function of P21 is to control the autonomic immune system and when neither of the switch functions can hydrolyze or glycolyze GTP, GDP, there is a free radical produced because the inability of the protein P21 to bind gamma phosphate leaves a residue identified as gamma phosphatase. The autonomic immune system responds to the gamma phosphatase, which is a free radical, with production of autoimmune antibodies that have been identified by Dr. D. Balomenos, of the Centro Nacional de Biotechnologia in Madrid, Spain. Dr. Balomenos has identified this autoimmune antibody as a multi-system auto-immune disease antibody known as human Lupus. |  | As
you note in this graph, P21 (H-Ras) is the dashed line with triangles. In the center is root canal extract at 5ul which inhibits this protein by 24% and at 40 ul, 67.6%. Remembering that anything over 12% renders P21 (H-Ras) to a nonfunctioning state. These
are terrible neurotoxins as you can see and being generated right in your own body! | 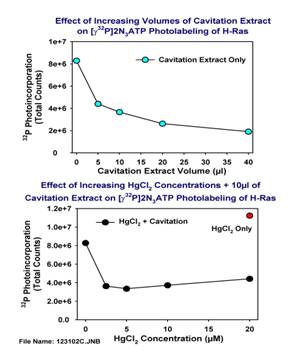 | At
5ul of cavitation extract, it is inhibited at 44.9% and then at 40ul this is increased to 76%. So, cavitation extracts totally inhibit P21 (H-Ras) ability to bind and function to CDK2. And as noted, the mercury reacts the same as shown in previous samples.
|  | You
will note that the bottom graph we also tested P21 (H-Ras) with the glio toxins. Inhibition due to glio toxins at 5um is 32.3%. At 20um, inhibition is at 55.7%. This protein P53 is severely inhibited.
|  | Now
we are looking at a graph where mercury from amalgams was added to the photo labeling gel. As you will note, photo labeling of the protein P21 increased with increasing amounts of mercury. So, mercury is not the cause of inhibition at this stage.
| | |
Now
we
have noted that all 3 proteins are greatly inhibited at even 5ul from being able to function properly, and that we have produced 3 distinct markers for the start of cancer: -
Inhibition
of
P53 due to these dental toxins which
makes it unable to suppress tumor start or growth. -
Inhibition
of
P21 which
causes uncontrolled cell replication. -
Inhibition
of
CDK2 which
creates uncontrolled cell growth. These
3
markers positively identify the diagnosis of any cancer! | 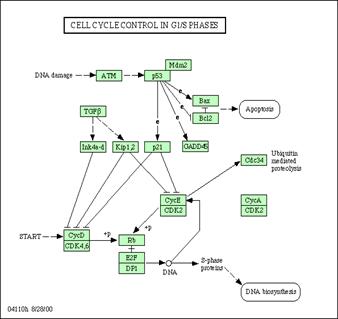 | Let
me present one more protein.
| | | CONCLUSION
OF THE CANCER PROTEINS Inhibition
of binding ability in all phases of GS1 of these three proteins expresses itself as the probable start of most, if not all, cancers. The chronic exposures of minute amounts of these toxins, which are also proven carcinogens, inhibit the binding ability of these proteins, which take on the form of a carcinogenic or mutant
cell until the carcinogenic dose is reached. The inhibited forms of P21, P53, P27 and CDK2 cannot function in the glycolyzation, hydrolyzation and methylyzation pathways and exhibit other "downstream" effects such as production of free radicals that are introduced into the bloodstream, which can lead to the production of antibodies exhibited in other auto-immune diseases such as lupus, Parkinson's, ALS and MS. Other
toxins that could cause this same condition have not been explored. More research is needed into inhibitions of these three proteins by chemical toxicants as a probable start of malignant growth and other downstream effects. This research believes that the lab findings are relevant to the start of cancer. Essentially,
there is no doubt that other neurotoxins exist in our environment but they are so rare, compared with the ones produced in our jawbones, that they are considered non-significant for the majority of cancer cases | |