| The only controls are the On/Off switch and Current output selector. To use the device just plug in the 15 volt AC adaptor (to wall socket and unit), select the lowest current setting (which means the device will output the labeled amount of milliamps of direct current), place the electrodes into the patient, make sure the output cable wires are securely connected to the electrodes, turn the unit on, and increase the output current if so desired. Please note that the insulator color at the end of the output wires indicate the polarity. The white insulator (shown in picture below) is indicating that this wire carries the positive voltage. The black insulator on the other wire indicates a negative voltage. 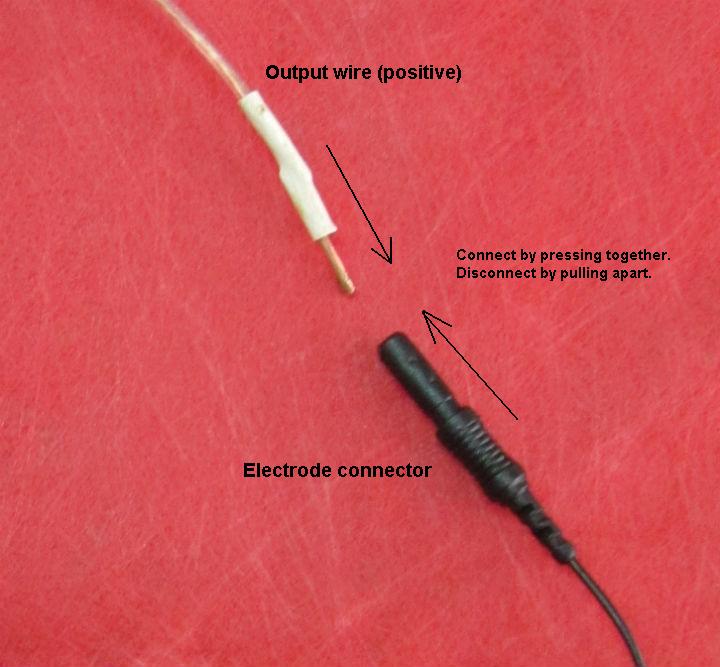 Nordenstrom admitted that a set optimal treatment method has not been realized yet so there is room for experimentation still. But the following gives us a general guideline of use by how others have used ECT successfully. Nordenstrom recommended that electrodes be neither very close nor very far away from one another. The anode (positive electrode) should be kept away from direct contact with large blood vessels if using the large currents and voltages. The cathode may be placed in a blood vessel. Nordenstrom used a catheter that could be percutaneously inserted by Seldinger technique in, for example, a pulmonary artery. Electrodes can theoretically be placed on the skin (although he cautions against this in a later paper) or inserted through a chest wall, via a systemic artery, a systemic vein, a bronchus or in the pleural space. The venous routes and pleural space provide pathways for current that include the lymphatics. Nordenstrom also noted that flushing the anodal electrode with a charged agent such as Adriamycin or 5-fluoracil in a manner that causes even distribution of the drug with high concentration can lead to a remarkable regression and palliative effects of even large, incurable cancers. Whether supplied intravenously or orally, these two agents are attracted to the electrode, when given opposite polarity. Nordenstrom treated 14 patients with otherwise incurable cancers with ECT and a chemotherapeutic agent Adriamycin infused into the tumor. The principle action is that an intramuscularly electropositive compound will be electrophoretically attracted to a neoplasm electrode given opposite polarity. This treatment was successful on larger tumors than was ECT alone and, in one case, abolished chronic cancer pain. Electrophoresis caused even distribution of the Adriamycin throughout the tumor, an effect probably not obtainable with injection. The above reports from China vary in the amount of technical detail presented regarding each study. In general, however, the electrodes were inserted under local anesthetic. The number of electrodes depended upon the tumor size and shape. The goal was to encompass the tumor with the electric field. With Xin et al the positive anode(s) was(were) placed within the tumor and the negative cathode(s) was(were) separated by from 1-3 cm from the anode(s) or by a distance from each other of 2-3 tumor diameters. There were a minimum of 2 electrodes and, at the other extreme, 2 anodes and 4-6 cathodes set up in two groups to establish two electric fields for a tumor of 6 cm or larger. The treatment time varied from 1.5-5 hours and the number of sessions ranged from 1 to 5, again depending upon tumor size and response to therapy. The voltage used averaged about 8V but ranged from 6 to 15 V. The current ranged from 40-100 mA and the number of coulombs delivered per session ranged from 250 to 2000. Quan gives a rule of thumb at 100 coulombs per 1 cm of tumor diameter. (100 coulombs is the equivalent of 50mA for 33 minutes or 40mA for 41 minutes, etc. See chart below.)
Song observed that at 100 coulombs the area of destruction around the anode is 0.5-0.6 cm and the area around the cathode is 0.4-0.5 cm. Xin et al observed some blockage of the heart beat in central lung cancer ECT with currents over 30 mA. Keeping the electrodes more than 3 cm from the heart corrected this effect. Electrotherapy is also believed to enhance the immune system of the patient (Chen et al., Chou et al). In studies conducted in mice there was infiltration of lymphocytes in tumor tissue six days after treatment. Leukocytes have a negative surface charge and are known to be sensitive to low voltage changes and changes in pH and ion strength. At an electrode voltage as low as 100 mV leukocytes concentrated at the anode. Many leukocytes can be attracted to the anode at relatively low voltages but are massively destroyed in the anodic field at 10 V. |